








Harm reduction – the current situation in Europe (European Drug Report 2026)

Harm reduction encompasses policies, programmes and interventions for reducing the health, social, legal and economic impacts of drug use on individuals, communities and societies. On this page, you can find the latest analysis of harm reduction interventions in Europe, including key data on opioid agonist treatment, take-home naloxone programmes, drug consumption rooms and more.
This page is part of the European Drug Report 2026, the EUDA’s annual overview of the drug situation in Europe.
Last update: 9 June 2026
Harm reduction is adapting to new and evolving drug problems
Illicit drug use contributes to the global burden of disease. Interventions to reduce this burden include prevention, which aims to delay or reduce drug use and its harms, and treatment to support stabilisation and recovery for people with drug-related problems. Harm reduction complements these approaches by working non-judgmentally with people who use drugs to reduce risks linked to their drug use behaviour and unsafe consumption conditions, and to promote health and well-being. A well-documented example is the provision of sterile injecting equipment to reduce the risk of infectious disease transmission. Measures such as this appear to have contributed to the low rate, by international standards, of new HIV infections associated with injecting drug use in Europe. Nonetheless, gaps in service provision and the growing use of stimulants present challenges for the European Union in meeting the WHO continuum-of-care targets among people living with HIV (see Drug-related infectious diseases – the current situation in Europe). In the last decade, evolving drug use patterns and changing user profiles have required harm reduction to address a wider range of risks. Harm reduction has expanded to include preventing overdoses linked to polysubstance use, responding to stimulant smoking and supporting vulnerable people facing complex health and social problems.
A spectrum of interventions is needed to tackle changing drug-related harms
Illicit drug use can cause chronic and acute health problems, potentially compounded by the properties of the substances, adulterants, route of administration, individual vulnerability and the social context of use. Chronic harms include dependence and infectious diseases, while the range of acute harms includes drug poisonings and overdoses. Although uncommon at the population level, opioid use accounts for much drug-related morbidity and mortality. Risks are higher with injecting and polysubstance use, making people who use opioids and inject drugs long-standing priorities for harm reduction interventions, with well-developed and evaluated service models.
Many harm reduction services, such as opioid agonist treatment and needle and syringe programmes are integrated into mainstream healthcare in Europe. Updated EUDA-ECDC guidance recommends combining opioid agonist treatment with the provision of sterile injecting equipment in community and prison settings to prevent the spread of HIV and hepatitis C, reduce injecting risk and maximise the coverage and effectiveness of these interventions among people who inject opioids.
Harm reduction equipment is usually delivered through integrated low-threshold services, which distribute sterile materials to reduce harms associated with continued drug use. The equipment provided may include items used for drug preparation and administration (e.g. filters, cookers, water, needles and syringes, pipes, foil) and items to prevent or respond to harms (wound care kits, naloxone) (Figure 13.1). Current evidence indicates the effectiveness of needle and syringe programmes and take-home naloxone, but evaluation data on other items remain limited, although observational studies suggest such provision can help broaden engagement with people who use drugs, including facilitating their access to treatment and social reintegration measures (Health and social responses: provision of harm reduction equipment for high-risk drug use).
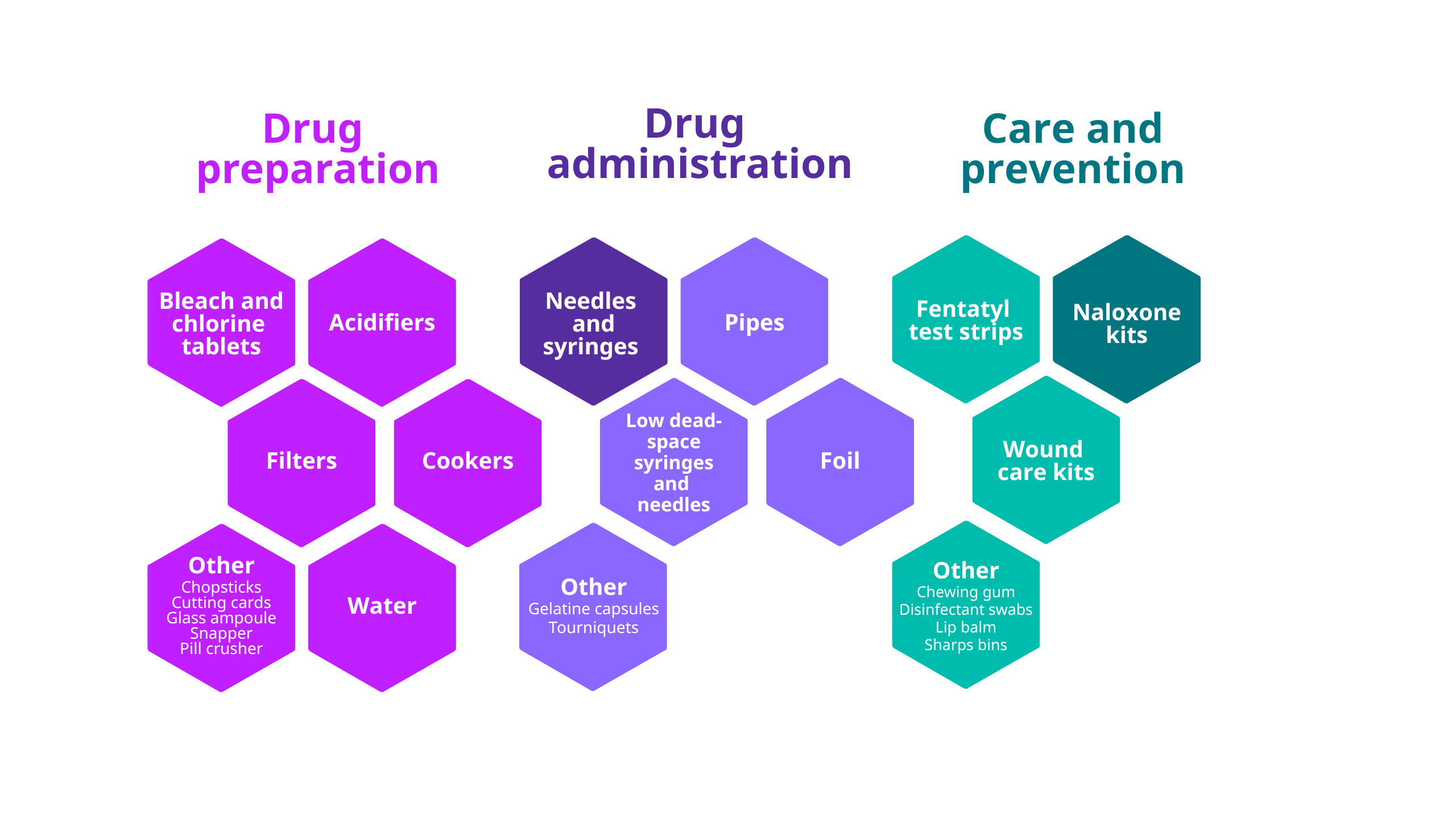
Show a text version of the above graphic
Drug preparation
- Bleach and chlorine tablets
- Acidifiers
- Filters
- Cookers
- Water
- Other: Chopsticks, cutting cards, glass ampoules, snappers, pill crushers
Drug administration
- Needles and syringes
- Pipes
- Low dead-space syringes and needles
- Foil
- Other: Gelatine capsules, tourniquets
Care and prevention
- Fentanyl test strips
- Naloxone kits
- Wound care kits
- Other: Chewing gum, disinfectant swabs, lip balm, sharps bins
Notes: Supplies for which there is evidence of benefit and where we can have a high or reasonable confidence in the available evidence are shown in a darker tone. Much of the current evidence on the provision of the supplies listed in this figure is either emerging or deemed insufficient (see Health and social responses: provision of harm reduction equipment for high-risk drug use and Spotlight on… Understanding and using evidence).
Harm reduction approaches have been broadened in some EU Member States to encompass additional responses. These include supervised drug consumption rooms and take-home naloxone programmes designed to reduce fatal overdoses (Figure 13.2). Interventions to reduce opioid-related deaths include measures aimed at tackling vulnerability, preventing overdoses from occurring and preventing fatal outcomes when overdoses do occur (Figure 13.3).
Show a text version of the above graphic
- Reducing fatal outcomes if overdose occurs
- Naloxone administration*
- Naloxone distribution and training* (specialist services and first responders, community)
- Drug consumption facilities*
- Fatal-overdose prevention apps
- Reducing the risk of overdose occurring
- Opioid agonist treatment, retention and continuity of care*
- Targeted interventions at times of reduced tolerance (e.g. release from prison or interrupted treatment)
- Overdose risk assessment, awareness raising and harm reduction
- Overdose prevention strategies
- Prevention of diversion of medicines
- Drug checking and public health alerts
- Supporting transition from injecting to smoking opioids
- Targeted treatments (naltrexone treatment, heroin-assisted treatment)
- Reducing vulnerability
- Integrated care with mental health and generic health services
- Interventions to improve access to social and health care
- Housing programmes
- Support to employment programmes
- Interventions to reduce or prevent stigma
Note: Interventions where there is evidence of benefit and where we can have high or reasonable confidence in the available evidence are highlighted in bold and marked with an asterisk (*).
Note: Interventions where there is evidence of benefit and where we can have high or reasonable confidence in the available evidence are highlighted in a bolder frame. Much of the current evidence on interventions listed in this figure is either emerging or deemed insufficient, in part because of the practical and methodological difficulties of conducting research, especially in developing randomised controlled trials (see Spotlight on... Understanding and using evidence) and also because service delivery models often differ considerably.
Drug consumption rooms provide supervised, hygienic spaces for people to use drugs. Sterile injecting equipment and safer use advice, including overdose prevention, are provided and staff can respond to on-site overdoses. These services may also link marginalised people with other harm reduction, treatment, healthcare and social services. They may also help reduce levels of public injecting. While evidence is still developing and evaluation is challenging, available data indicate that drug consumption rooms can contribute to reducing drug-related deaths (see also Health and social responses: drug consumption rooms).
Take-home naloxone programmes provide overdose risk and response training and distribute naloxone kits to people likely to witness an opioid overdose. While increasing numbers of individuals have been trained in administering naloxone, coverage and access issues still exist in some in EU Member States providing the intervention (see Opioid-related deaths: health and social responses).
In some countries, drug checking services allow people to understand what the illicit drugs they have bought contain. With many synthetic stimulants and new psychoactive substances now available on the illicit market in similar-looking powders or pills, consumers may be unaware of what they are consuming. When offered within drug consumption rooms, drug checking can reach more vulnerable groups and may help reduce overdose risk linked to unexpected or potent opioids. Drug checking services provide insights into current drug market trends and consumer preferences, ultimately supporting targeted risk communications and alerts (see also Synthetic stimulants – the current situation in Europe and MDMA – the current situation in Europe).
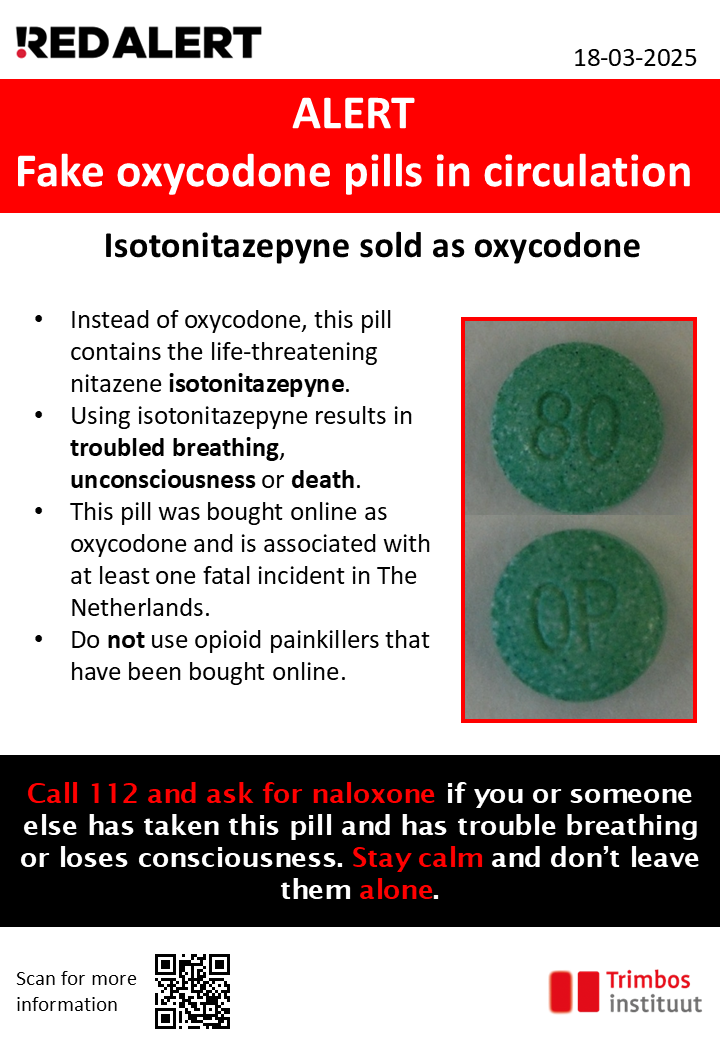
The increased integration of the markets for new psychoactive substances and illicit drugs has created new public health challenges. Examples include hemp mixed with synthetic and semi-synthetic cannabinoids; stimulants mixed with various substances, sometimes including synthetic cathinones; ketamine; or new synthetic opioids (e.g. nitazenes) mixed with or mis-sold as heroin (see also New psychoactive substances – the current situation in Europe). As poisoning events can evolve rapidly, risk communication has become more important. For example, when isotonitazepyne, a potent nitazene opioid mis-sold as oxycodone tablets, was linked to a fatal overdose in the Netherlands in March 2025, a rapid risk alert communication was issued to warn unsuspecting opioid consumers who may have purchased similar tablets (Figure 13.4). Events like this underline the need for coordinated systems such as the EUDA’s new European Drug Alert System, which supports EU and national preparedness and response activities to serious drug-related risks through rapid information exchange, targeted alerts and other risk communications. Given developments in the synthetic opioids market, preparedness planning will be important and can focus on enhancing toxicological capacity, alert messaging and supporting the readiness of frontline health and social services.
Growing stimulant use highlights gaps in harm reduction service provision
HIV outbreaks associated with the injection of illicit stimulants have been documented in 7 European cities, across 6 EU Member States during the last decade. Stimulant use is associated with a potentially higher frequency of injection compared with heroin use, while crushing and dissolving crack cocaine and other tablets for injection also brings with it additional health risks. High levels of harm reduction service coverage are needed to prevent and rapidly contain infectious disease outbreaks.
Synthetic stimulants and other substances are sometimes consumed to facilitate and enhance sex in the context of sexualised drug use, known as ‘chemsex’, by various groups but mainly among a small sub-population of men who have sex with men. Engaging with and providing effective harm reduction responses for this group is challenging due to a lack of integrated service provision, tailored harm reduction interventions and limited knowledge of the prevalence of this pattern of use. Addressing this issue requires strong multi-agency partnerships between sexual health services and harm reduction services.
Diverse drug problems highlight the need to scale up harm reduction services
Despite cannabis being Europe’s most consumed illicit drug, harm reduction advice and interventions are often lacking. Cannabis resin and herb are typically of higher potency than in the past and are associated with more acute and chronic harms. Greater product diversity, with edibles, e-liquids and extracts available, alongside increased availability of semi-synthetic cannabinoids, complicates the identification and implementation of effective harm reduction interventions in this area.
Various other substances present additional harm reduction provision challenges. Among these are the unpredictable health effects posed by new psychoactive substances appearing in powders or used in e-liquids for vaping. While difficult to quantify, the potential risk of bladder damage from ketamine use and risk of spinal cord degeneration and peripheral neuropathy from vitamin B12 deficiency induced by the use of nitrous oxide canisters present emerging challenges to harm reduction, treatment and linkage to services (e.g. urology, neurology).
Across the European Union, coverage and access to harm reduction services vary widely and remain below estimated needs in some countries. Rapidly changing drug markets, characterised by more complex use patterns, new substances and mixtures, and risks concentrated in specific groups or settings, underline the need to further develop and evaluate responses such as drug consumption rooms and drug checking services. The EUDA’s Health and social responses to drug problems: a European guide provides more information on the evidence for harm reduction and other interventions.
Key data and trends
Needle and syringe programmes
- In 2024, needle and syringe programmes were in place in all EU Member States and Norway. Only 7 of the 25 countries with available data had reached the 2025 WHO service provision target in 2024 (Figure 13.5); only 4 of these countries also provide data on the coverage of opioid agonist treatment.
Opioid agonist treatment
- In 2024, of the 22 countries with available data, 14 had reached the 2025 WHO service provision target for opioid agonist treatment (Figure 13.5); only 9 of these also provide data on the coverage of needle and syringe provision.
- A range of opioid agonist medications are prescribed in Europe, with methadone received by 61% of opioid agonist treatment clients, while another 36% receive buprenorphine.
Take-home naloxone programmes
- Up to 2025, take-home naloxone programmes were available in 19 European countries (Figure 13.6).
- The number of naloxone kits distributed by take-home programmes was reported by 10 of the 19 countries for 2024, with 8 reporting an increase compared with 2023.
- Naloxone was used as a nasal spray in 17 of these countries and injectable naloxone formulations were used in 7 countries.
- Injectable naloxone 0.4 mg/1 ml vials (as included in the WHO essential medicines list) were used in five countries: Ireland, Spain, Italy, Lithuania and Portugal.
- Naloxone is available over the counter in Denmark, France, Italy, Sweden and Norway.
Drug checking services
- Eleven European countries reported the provision of some type of drug checking service in 2025 (12 in 2024). The services use various techniques (Figure 13.7) and operate in a range of settings, including festivals, drug consumption rooms and at fixed locations in the community.
Drug checking technologies ranked in order of increasing accuracy and reliability of results:
- Multiple methods
(most accurate and reliable) - High-performance liquid chromatography
- Fourier transform spectroscopy
- Thin-layer chromatography
- Reagent test kit
(least accurate and reliable)
Drug consumption rooms
- In 2025, a total of 100 drug consumption rooms were operational in 13 EU Member States and Norway (Figure 13.8). Service provision includes supervised injecting, supervised use of stimulants (e.g. smoking crack), drug checking, provision of hygienic equipment and other forms of health and social support.
Interventions in prisons
- EUDA data on harm reduction and treatment interventions available in prisons in 2024 show that continuity of opioid agonist treatment between the community and prison settings was available in all but one EU Member State (Slovakia), and in Norway and Türkiye. Initiation of opioid agonist treatment in prison was not allowed in 3 countries (Bulgaria, Latvia, Slovakia). Needle and syringe programmes were available in prisons in 4 countries: in all prisons in Spain and Luxembourg (1 prison), in 10 prisons in France and in 1 prison for women in Germany. Naloxone provision upon release from prison was available in 10 countries in 2024 (Germany, Estonia, Ireland, Greece, France, Croatia, Italy, Luxembourg, Slovenia, Norway). The number of countries reporting the official availability of selected harm reduction interventions (Figure 13.9) increased in 2024 compared with 2023.
- In 2025, ECDC and the EUDA jointly launched a toolkit for the elimination of viral hepatitis in prison.
Number of countries where the intervention was officially available in 2024
Source data
The data used to generate infographics and charts on this page may be found below.
The complete set of source data for the European Drug Report 2026, including metadata and methodological notes, is available in our data catalogue.
A subset of this data, used to generate infographics, charts and similar elements on this page, may be found below.