








Non-medical use of medicines: health and social responses
Introduction
This miniguide is one of a larger set, which together comprise Health and social responses to drug problems: a European guide. It provides an overview of the most important aspects to consider when planning or delivering health and social responses to problems related to the non-medical use of medicines, and reviews the availability and effectiveness of the responses. It also considers implications for policy and practice.
Last update: 20 October 2021.

Contents:






Overview
Key issues
There is a growing recognition of the important public health consequences that can arise as a result of the non-medical use of medicines and medicinal products. Problems associated with the non-medical use of medicines include both acute health harms and chronic problems, such as dependence.
The groups of medications that have most commonly been associated with concerns about their non-medical use in the EU include:
- sedatives and hypnotics, including barbiturates, benzodiazepines and benzodiazepine-like drugs such as the ‘Z-drugs’;
- opioids, including pain relief medications and opioid agonist treatment medications;
- stimulants prescribed to treat attention deficit and hyperactivity disorder (ADHD); and
- over-the-counter drugs, including some cough syrups and antihistamines.
The diversion and non-medical use of opioid agonists is of particular concern in Europe. In addition to mortality, related consequences include complications associated with the injection of the medication, a negative impact on treatment outcomes, and threats to the reputation of treatment services.
Evidence and responses
- Monitoring to establish the extent and nature of the problem is essential in developing appropriate responses.
- Good clinical practice, supported by clear guidelines, can lower the risk that medicines may become diverted and misused. In the case of opioid agonist medications, it can also reduce the harms associated with their non-medical use.
- Prevention approaches include practitioner training and the establishment of quality standards and protocols to improve prescribing practice; controls on availability, such as limiting sales and imposing packaging restrictions, along with introducing disposal schemes for waste or surplus medicines; and the use of formulations that are designed to deter non-medical use.
- Ensuring that healthcare professionals are trained in identifying and treating problematic use, and know how to address signs of non-medical use. Offering support in primary care settings may be appropriate for people with problems associated with the non-medical use of medicines who may be reluctant to seek help from traditional drug treatment services.
European picture
- Information is limited on the current treatment practices in Europe for managing the non-medical use of medicines. This hampers both the assessment of trends and the targeting of responses.
- Work to better understand the extent and nature of the problem and monitor developments is underway and includes the monitoring of acute events through sentinel sites (by Euro-DEN Plus), the collection of data from drug-checking services and developing wastewater analysis.
- There have been several EU-funded projects in this field, such as CODEMISUSED looking at Codeine Use, Misuse and Dependence, the Access To Opioid Medication in Europe (ATOME), and the ongoing collaboration between the EMCDDA and the European Medicines Agency around the non-medical use of opioids in Europe.
Key issues: patterns of non-medical use of medicines and related harms
Key questions that need to be addressed when identifying and defining a problem include who is affected, what types of substances and patterns of use are involved, and where the problem is occurring. Responses should be tailored to the particular drug problems being experienced, and these may differ between countries and over time. The wide array of factors that have to be considered at this stage in the process are discussed in the Action framework for developing and implementing health and social responses to drug problems.
The non-medical use of prescription medicines is a matter of increasing concern in Europe and is associated with a range of both acute health harms and chronic problems, such as dependence.
Many substances controlled under the international drug control conventions have medical uses, and a stated aim of the international drug control system is to ensure the adequate availability of essential medicines while at the same time introducing measures to reduce the possibility of their being used inappropriately.
Medicinal substances also have a long history of appearing on the drug market and being trafficked or used because of their psychoactive properties. Overall, however, compared to other substances, the current understanding of patterns and trends in this area is often more limited. There are a number of reasons for this, including the large number of medicines that have psychoactive properties; the definitional complexity of what constitutes non-medical use (see Spotlight on… Non-medical use of benzodiazepines);; and the fact that these medicines are often used alongside more well-known illicit drugs (in a polydrug use context).
Information from the European Drug Emergencies Network (Euro-DEN Plus),
The majority of medicines are prescribed according to standard practice and guidelines, often for a limited period. Problems may arise when people continue to use them after the original health issue has been resolved, use too much or increase the amounts taken beyond the therapeutic dosage, or allow them to be used by family members or friends. In addition, the non-medical use of medicines in combination with other drugs or medicines can lead to interactions that may increase harms and even result in death.
The following are some common patterns of non-medical medicine use:
- Some people with anxiety disorders and other mental health problems or pain may use medicines to self-medicate these symptoms without appropriate medical supervision or outside of accepted medical practice.
- Some people who have no medical reasons for using medicines use them for recreational or enhancement purposes, for example to obtain a high, improve their physique or facilitate concentration for long periods.
- Many people who use heroin or central nervous system stimulants also use prescription opioids. Benzodiazepines or ‘Z-drugs’ may also be used to increase the high, postpone opioid withdrawal or reduce the adverse symptoms occurring after consuming stimulants (anxiety, depression, sleeplessness, etc.). This type of polydrug use can also be considered a form of self-medication in people who use heroin and stimulants.
The diversion and non-medical use of opioid agonist medications (such as methadone and buprenorphine) is an issue of particular concern in Europe. The number of deaths associated with these medications, although not necessarily diverted from therapeutic use, has been increasing over the last decade in a number of countries. In addition to mortality, the consequences of the non-medical use of opioid agonist medications include somatic complications associated with the injection of the medication (e.g. limb ischemia or tissue necrosis) as well as the risk of contracting blood-borne viruses and a potential negative impact on treatment outcomes. Concerns about the diversion of opioid agonist medications may also have a negative impact on prescribers’ practice, threaten the reputation of treatment services and compromise public acceptance of the long-term treatment of opioid-dependent individuals. Some studies have shown that good clinical practice supported by prescribing guidelines may reduce the risk of these medicines being inappropriately used within the community.
European data and studies suggest that the majority of individuals using prescribed or non-prescribed opioid agonist medications for non-medical purposes in Europe are also engaged in long-term, high-risk opioid use and have a history of opioid dependence and treatment experience.
One important driver of the non-medical use of medicines is poor prescription practice. This includes over-prescription but also, particularly in the case of opioid agonist medication, under-prescription. Suboptimal prescribing practices may be contributing to a growing demand for diverted opioid agonist medications among patients to ‘top up’ their prescribed dosage and achieve effective opioid levels, or they may use illicit opioids for this purpose. Inadequate or conservative opioid agonist dosages (not in line with recommended doses in clinical guidelines) have been documented in a number of European countries. Lack of access to opioid agonist treatment is another recorded reason for the non-medical use of opioid agonist medications (see also the EMCDDA Technical report Balancing access to opioid substitution treatment (OST) with preventing the diversion of opioid substitution medications in Europe: challenges and implications).
Evidence and responses to problems related to the non-medical use of medicines
Choosing responses that are likely to be effective in dealing with a particular drug-related problem requires a clear understanding of the primary objectives for the intervention or combination of interventions. Ideally, interventions should be supported by the strongest available evidence; however, when evidence is very limited or unavailable, expert consensus may be the best option until more conclusive data is obtained. The Action framework for developing and implementing health and social responses to drug problems discusses in more detail what to bear in mind when selecting the most appropriate response options.
In considering responses to the non-medical use of medicines, it is important to adhere to what the World Health Organization (WHO) describes as the principle of balance, which stresses the need to minimise the non-medical use of medicines while maximising their availability for appropriate medical use.
Monitoring
Increasing our understanding of the extent and nature of the non-medical use of medicines, including the monitoring of prevalence, motivations for use, systemic barriers to accessing treatment, and sources of supply, as well as monitoring changes over time, is essential for developing appropriate responses. However, the diversity of medicines and their sources of supply as well as the different groups who use them, along with variations between countries in prescribing practice and legal frameworks, make this a challenging task. This diversity also means that it is important to clearly define what constitutes non-medical use, particularly for cross-national comparisons.
The extent of the problem needs to be assessed using a variety of data
Indications of the non-medical use of medicines may also come from national or international databases on adverse drug effects. Other sources of information include autopsies and
Pharmacy sales statistics represent a cheap and efficient way to follow medicine use and trends. Health insurance claims and prescription databases can also provide useful information. Data from these sources can further be analysed to provide information on the extent of doctor shopping and forged
Monitoring the internet can also help to flag the non-medical use of medicines. Data can be collected from websites on trends in information requests about specific medicines or from online reports of non-medical use.
Prevention and treatment
Measures for the prevention and treatment of the non-medical use of medicines must ensure the availability of medicines for people who need them for medical reasons while minimising the scope for their non-medical use. For this purpose, the WHO has developed guidelines on access to controlled medicines. Lack of such access is a problem in a number of countries globally, including some in Europe.
The increasing availability of medicines over the internet poses challenges to regulation and will require the development of new responses. Many of these, as is often the case for actions against diversion at the production and distribution stages of supply, will involve law enforcement rather than health and social responses. A clearer understanding of the sources of the medicines appearing on different markets will be crucial for success here.
In recent years, a number of technological advances have reduced the opportunities for some forms of diversion. For example, the introduction of electronic record keeping and centralised prescription databases has limited the opportunities for doctor shopping.
As opioid agonist treatment can also be a potential source of diversion, good clinical practice needs to strike a balance in ensuring that there is sufficient and easy access to opioid agonist treatment for all those that require it, delivered at clinically appropriate doses, while at the same time suitable safeguards exist to reduce the risk of possible diversion. As the US opioid epidemic appears to have been driven in part by the inappropriate prescribing of pain medications, attention is also needed to ensure the existence of guidelines and that clinicians are aware of the potential negative consequences of inappropriate prescribing of medicines intended for pain relief.
One strategy to prevent the diversion of opioid agonist medications is to register patients undergoing this treatment, and in some countries one central register records all patients at the national level. This has a number of advantages: it prevents patients from receiving methadone, buprenorphine or other opioid agonist medications from more than one source; it can be used to limit access to other controlled medicines requiring central approval, such as other opioids; and it can provide more accurate data on treatment numbers. However, a potential disadvantage of the central registration of patients is that it can risk breaches of privacy, and this may deter some patients from entering treatment. According to WHO guidelines, safe and effective treatment of opioid dependence can be achieved without central registration. Because such registration could cause harm if privacy is breached, it should be used only if government agencies have effective systems for maintaining privacy and controlling personal data sharing.
Although the diversion of opioid agonist medications has been described as a growing problem in recent years, there has been little systematic monitoring of the extent and nature of the problem. Therefore additional empirical data is needed to inform regulatory decisions and develop prevention and risk management plans.
The treatment for the non-medical use of medicines is similar to that for other drug use disorders and has to be tailored to individual needs. Current evidence supports the use of cognitive behavioural therapy to reduce dependence on benzodiazepines, alongside tapering the dosages of these substances, but results have only shown this to be effective in the short term. Cognitive behavioural therapy interventions promote the development of alternative coping skills and aim to change behaviours and cognitions related to substance use through focusing on self-control, social and coping skills and relapse prevention. There is also evidence to suggest that opioid agonist treatment may be effective in improving treatment retention and reducing substance use in people who are dependent on pharmaceutical opioids.
People experiencing problems associated with the non-medical use of medicines come from a wide range of
A strong therapeutic relationship between the patient and physician can play an important role in preventing the non-medical use of medicines. In dealing with patients who use drugs, doctors need to be aware of the reasons patients give when requesting additional prescriptions, such as lost medicines and prescriptions and, if frequently repeated, investigate further. They should be cautious in prescribing to unknown patients, while not withholding medication from patients in need. Primary healthcare workers need to be trained to deal with these dilemmas.
Overview of the evidence concerning … treatment for non-medical use of medicines
| Statement | Evidence | |
|---|---|---|
| Effect | Quality | |
| Cognitive behavioural therapy helps to reduce the use of benzodiazepines when added to the tapering dosages of these substances, but only in the short term. | Beneficial | Moderate |
| Buprenorphine and methadone agonist treatment are both effective in improving retention in treatment and reducing substance use in people who are dependent on pharmaceutical opioids | Beneficial | Low |
Evidence effect key:
Beneficial: Evidence of benefit in the intended direction. Unclear: It is not clear whether the intervention produces the intended benefit. Potential harm: Evidence of potential harm, or evidence that the intervention has the opposite effect to that intended (e.g. increasing rather than decreasing drug use).
Evidence quality key:
High: We can have a high level of confidence in the evidence available. Moderate: We have reasonable confidence in the evidence available. Low: We have limited confidence in the evidence available. Very low: The evidence available is currently insufficient and therefore considerable uncertainty exists as to whether the intervention will produce the intended outcome.
European picture: availability of interventions related to the non-medical use of medicines
A number of international organisations and agencies have responsibilities in the area of medicines control, including the European Medicines Agency, the World Health Organization, the United Nations Office on Drugs and Crime, and the International Narcotics Control Board. The EMCDDA collects information on national legislation that covers prescribing, authorised substances and prescription regulations, plus any criteria for enrolment in opioid agonist treatment and sanctions for infractions.
Substitution registers in EU Member States help to prevent patients receiving multiple prescriptions, which can arise when two or more doctors prescribe in parallel. Other psychoactive -medicines, such as
Services such as the EudraVigilance database maintained by the European Medicines Agency, and the WHO’s adverse effects database may also capture indications of the non-medical use of medicines. These agencies compile data on substances associated with adverse events reported by hospital emergency departments and other sources. They include information on problems associated with medicines taken for recreational purposes alone or with other psychoactive substances.
In addition, the European Drug Emergencies Network (Euro-DEN Plus) monitors drug-related emergency presentations in 31 sentinel centres across Europe, providing unique insights into acute health harms related to drug use and also in relation to the non-medical use of medicines.
A number of European research projects are relevant to this area, including the completed EU-funded project ATOME (Access To Opioid Medication in Europe) and CODEMISUSED, a 4-year EU-funded project looking at codeine use, misuse and dependence (2013-2017). The EMCDDA is currently cooperating with the European Medicines Agency and other international partners around the non-medical use of opioids in Europe, with a particular focus on monitoring the illicit opioid market.
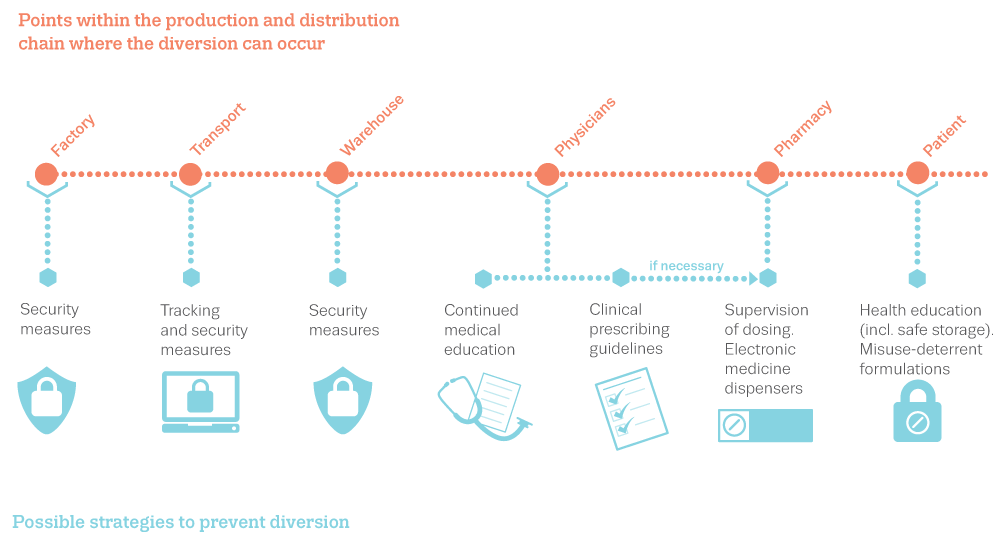
A number of interventions have been developed and are currently used in Europe to minimise the diversion of opioid agonist medications. These include:
- clinical prescribing guidelines on the supervision of doses for people who are not stable in terms of their treatment;
- educating physicians on safe opioid prescribing, including comprehensive initial assessment and regular monitoring of patients, and providing information to patients on safe use, including appropriate storage and disposal;
- electronic medicine dispensers to promote safe opioid prescribing and reduce medical errors;
- control measures such as patient toxicology tests, pill counts and unannounced monitoring;
- regulation at system level via registers of pharmacy transactions, with disciplinary measures to address inappropriate
- the use of non-medical use-deterrent formulations, for example suboxone, or the dilution of methadone to discourage injection.
When implementing such measures, it is important to consider potential unintended consequences, for example, where reductions in access to prescribed medications due to strict controls may result in patients turning to illicit sources of supply to self-medicate.
In many EU Member States, especially in eastern European countries, physicians have to use special prescription forms, often in multiple copies, to provide information to the central registration system. These forms are not always free of charge and doctors authorised to prescribe can face complex reporting requirements, perceived as delaying the commencement of treatment and deterring practitioners from engaging in opioid agonist prescribing. The majority of Member States have only one specific registry recording patients receiving opioid agonist treatment. These registries are often located in national health departments or institutes or national medicines agencies.
While European countries may have some commonalities, many patterns of use, motives and drivers for the non-medical use or diversion of medications appear to be country-specific. For example, some countries with limited access to opioid agonist treatment report relatively high numbers of drug-related deaths that mention opioid agonist medications, or sizable law enforcement agency seizures. Large-scale opioid agonist treatment provision is therefore unlikely to be the main driver of diversion and non-medical use in these countries. In some other countries, the diversion and non-medical use of these medications may be facilitated by high opioid agonist treatment accessibility or liberal therapeutic supervision and limited monitoring of prescribing.
For these reasons, ‘one size fits all’ recommendations and policies to prevent diversion and reduce the levels of non-medical use will most likely be ineffective in addressing the specific national causes of the observed problems. In each country, the design and implementation of such measures will present difficult trade-offs, as the advantages of offering easily accessible, effective and user-customised treatment for a large group of individuals must be weighed against the negative effects of diversion.
Implications for policy and practice
Basics
Core objectives in this area include:
- Ensuring that prescription medicines likely to be used for non-medical purposes are sufficiently available to meet legitimate needs, while limiting the opportunities for diversion.
- Ensuring that healthcare professionals are given correct prescribing guidelines and practical training in identifying and treating problematic use, as well as addressing signs of non-medical use.
Opportunities
- Develop and provide alternative treatment options to deal with the non-medical use of medicines for patients who are reluctant to seek help in traditional drug dependence treatment settings.
- Promote awareness among patients and the general population about the non-medical use of medicines in order to destigmatise the problem and encourage people to seek help.
- Work with clinicians and pharmacists to increase awareness and promote good clinical practice.
Gaps
- Investigate and monitor the extent and nature of the non-medical use of medicines in order to facilitate the development of appropriate interventions, using a wide range of sources.
- As medicines are often used in combination with other substances, monitoring and research needs to become more sensitive to reporting on the concurrent use of substances, critical drug combinations and potential public health implications. In particular, investments should be made in:
- studies of drug users to understand the types of medicines being taken and the contexts in which use occurs;
- improving toxicological monitoring of fatal and non-fatal overdoses to gain a better insight into the range of drugs involved and any significant drug interactions or combinations; and
- clinical studies to improve understanding of effective treatment approaches in this area.
Further resources
EMCDDA
- Best practice portal.
- EMCDDA activities in the area of hospital emergency data.
- Balancing access to opioid substitution treatment (OST) with preventing the diversion of opioid substitution medications in Europe: challenges and implications, Technical report, 2021.
- New benzodiazepines in Europe – a review, Technical report, 2021.
- European Drug Report 2021: Trends and Developments.
- Strategies to prevent diversion of opioid substitution treatment medications, Perspectives on drugs, 2016.
- The misuse of benzodiazepines among high-risk opioid users in Europe, Perspectives on drugs, 2015.
Other sources
- World Health Organization, Ensuring balance in national policies on controlled substances: guidance for availability and accessibility of controlled medicines, 2011.
- INCB, Availability of Internationally controlled drugs: ensuring adequate access for medical and scientific purposes. Indispensable, adequately available and not unduly restricted, 2015.
About this miniguide
This miniguide provides an overview of what to consider when planning or delivering health and social responses to problems related to the non-medical use of medicines, and reviews the available interventions and their effectiveness. It also considers implications for policy and practice. This Miniguide is one of a larger set, which together comprise Health and social responses to drug problems: a European guide.
Recommended citation: European Monitoring Centre for Drugs and Drug Addiction (2021), Non-medical use of medicines: health and social responses, https://www.emcdda.europa.eu/publications/mini-guides/non-medical-use-o….
Identifiers
HTML: TD-08-21-221-EN-Q
ISBN: 978-92-9497-668-0
DOI: 10.2810/679602
[1] The term opioid agonist treatment is used here as preferred language to cover a range of treatments that involve the prescription of opioid agonists to treat opioid dependence. The reader should be aware this term includes opioid substitution treatment (OST), which may still be used in some of our data collection tools and historical documents.