








Drug-related infectious diseases – the current situation in Europe (European Drug Report 2025)
People who inject drugs are at risk of contracting infections through the sharing of drug use paraphernalia. On this page, you can find the latest analysis of drug-related infectious diseases in Europe, including key data on infections with HIV and hepatitis B and C viruses.
This page is part of the European Drug Report 2025, the EUDA’s annual overview of the drug situation in Europe.
Last update: 5 June 2025
Infectious diseases related to drug use remain a challenge
People who inject drugs are at high risk of becoming infected by hepatitis B and C viruses (HBV and HCV, respectively) and the human immunodeficiency virus (HIV) through the sharing of drug use paraphernalia. These infections can cause chronic diseases that may result in severe health-related harms, including death.
Harm reduction gaps and stimulant use hinder EU reaching HIV Sustainable Development Goals
New HIV notifications are an indicator of both the level of viral transmission and also of the corresponding level of prevention interventions required. While the total number of HIV notifications in the European Union linked to injecting drug use declined to 980 in 2023 (1088 in 2022), the notification rate of 2.18 per million population remained at pre-COVID-19 pandemic levels (Figure 10.1). This may be in part due to a return to previous levels of service, and the increased movement of people living with a known HIV diagnosis in European countries following the full-scale Russian invasion of Ukraine may also have contributed. These data need to be interpreted with caution, as they are not necessarily indicative of an increase in rates of new infections. Nor do they necessarily put into question the long-term decline in HIV notifications.
Harm reduction approaches are now seen as fundamental to reducing HIV transmission among people who inject drugs, particularly the provision of sterile injecting equipment, including in prisons and through pharmacies. Nonetheless, several issues now underline the need for renewed efforts within the European Union to enhance services to counter the burden of infectious diseases and sustain the gains made against HIV transmission in earlier years. Among these are the decreasing availability of sterile injecting equipment in some countries and inadequate geographic coverage. Available data show that in two thirds of EU Member States, the annual average number of sterile syringes distributed per person who injects drugs remains below the WHO target and, in some cases, has decreased (Figure 10.2). Also, the geographical coverage (Figure 10.3) of the provision of sterile syringes remains inadequate in several countries, including Bulgaria, Croatia, Cyprus, Lithuania, Hungary, Malta, Poland, Romania and Slovakia. In Bulgaria, where harm reduction funding and procurement difficulties persist, drug treatment services reported a marked increase in the HIV positivity rate, a proxy measure for HIV prevalence, among people who inject drugs, reaching 16 % in the capital Sofia in 2023. In addition, Europe continues to observe an increased availability of various stimulant drugs, including cocaine, amphetamine, synthetic cathinones and, to a lesser extent, methamphetamine. The injection of stimulant drugs is associated with more frequent and damaging patterns of injecting drug use. Over the last decade, Europe has witnessed at least seven documented HIV outbreaks that were attributable to stimulant injecting (Figure 10.4). As the availability of stimulants continues to increase, the risk of further outbreaks adds to the challenges for HIV prevention posed by Europe’s longstanding opioid problems. Lastly, Europe’s experience with HIV outbreaks related to stimulant injection has shown that relatively high levels of harm reduction service provision are required to prevent and contain such events. The implication of this is that countries with inadequate service levels with respect to the size of their estimated injecting drug use problems remain more exposed to potential HIV outbreaks.
Alongside outbreak preparedness, linking all people who use drugs who are HIV-positive to treatment remains a challenge within the European Union. Estimates from seroprevalence studies conducted between 2021 and 2023 showed HIV prevalence among people who inject drugs above 15 % in Estonia, Greece, Latvia, Lithuania, Poland and Romania. The WHO targets for the continuum of care among people living with HIV aim to have 95 % of people living with HIV tested, 95 % of these people on antiretroviral therapy and 95 % of those achieving viral suppression by 2030, to support achieving the Sustainable Development Goals. In 2023, EU Member States reported 186 AIDS notifications linked to injecting drug use (0.41 per million population), indicating either late HIV diagnosis, poor treatment access or low adherence for some patients, which contribute to preventable illness and death. The AIDS notifications rates linked to injecting drug use were higher than 1 per million in Bulgaria, Greece, Cyprus, Latvia, Lithuania and Romania, indicating major gaps in the HIV continuum of care for this key population.
City-level reduction of chronic drug-related HCV infection
In Europe, people who inject drugs also have a high burden of chronic viral hepatitis, and injecting drug use remains the most common risk factor for new HCV diagnoses. A recent study found that at least 36 % of the overall chronic HCV prevalence in the EU Member States, Norway and Iceland is associated with injecting drug use. There is also evidence that harm reduction services, such as needle and syringe programmes, as well as the provision of opioid agonist treatment, can reduce the risk of HCV transmission. As noted earlier, the coverage of and access to these interventions vary considerably between European countries (Figure 10.3). In addressing the harms associated with HCV infection, it is important to identify individuals who remain chronically infected with the virus, as they are at risk of cirrhosis and cancer, and can transmit the virus to others through the sharing of any injecting paraphernalia that has been in contact with their blood. However, barriers to the uptake of HCV testing and treatment exist in many countries and may result in many HCV infections not being diagnosed and treated.
Time trends in the prevalence of viraemic or active HCV infection among people who inject drugs are useful for monitoring the impact of prevention and treatment. The EUDA monitors progress through its viral hepatitis elimination barometer. Among the countries reporting to the EUDA, Spain, Sweden and Norway have evidence of significant reductions in viraemic HCV prevalence over time, as measured by HCV-RNA in city-level seroprevalence studies among people who inject drugs and use harm reduction services. In Stockholm, it decreased from 64 % in 2015 to 30 % in 2021; in Madrid, it decreased from 41 % to 20 % between 2015 and 2022. The largest reduction was observed in Oslo, where it decreased from 46 % in 2015 to 7 % in 2023, thus reaching the 80 % reduction target set by WHO. In Luxembourg’s main prison – a setting where drug use is a common source of HCV exposure – the prevalence of HCV-RNA on admission screening decreased from 10 % in 2015 to less than 5 % in 2021. These encouraging trends are reported from cities where a decentralised and integrated approach to prevention, testing and treatment has been implemented for the key population of drug users. Different aspects of this approach, endorsed in the joint EUDA-ECDC guidelines (see below), are present across the cities with, for example, Madrid providing increased access to harm reduction for outreach service clients and offering free testing and personalised referrals to care when a hospital visit is required. In Stockholm, testing and treatment offers are, as much as possible, made in the same location. Luxembourg aims to ensure that those receiving a diagnosis while in prison complete treatment and are linked to post-release health services. Overall, the decentralised and integrated approach aims to maintain high coverage of prevention and harm reduction provision to prevent re-infections. While this approach requires sufficient financial resources, it is considered cost-effective in many ways, as it can save lives and reduce the burden on other resources in the long term.
Clusters of sexually transmitted infections highlight need for integrated care for people who use drugs
Recently, a cluster of syphilis, a sexually transmitted bacterial infection, was detected among people who use drugs in Luxembourg. In total, 23 cases were detected between November 2023 and September 2024. Among the cases were eight women, some of whom had reported being involved in sex work to finance their drug use and were considered marginalised and had not been in contact with mainstream healthcare services. Despite Luxembourg’s overall high level of harm reduction services, the emergence of this cluster of infections and its links to drug use highlight the vulnerability of marginalised populations that may not be in contact with services. It also shows that if a HIV outbreak investigation had not been conducted, the infection cluster may have remained undetected. This in turn raises the possibility that there are similar clusters that have not been detected.
In other populations, the use of illicit stimulants and other drugs to facilitate group sexual encounters, sometimes of an extended duration, among a small sub-population of men who have sex with men is known as chemsex. The drugs associated with this practice include synthetic stimulants, depressants and dissociatives, and both high-risk drug-taking and high-risk sexual behaviours may overlap, making this an important area for outreach and harm reduction. High-risk use of some of these drugs, including by injection, places people at risk of infectious diseases. This includes blood-borne viruses such as HIV and HCV, but also other diseases such as mpox, shigella and hepatitis A, clusters of which were detected among men who have sex with men in several EU Member States in 2023. It also places users at higher risk of acute drug toxicity and other health problems. People using drugs in this way often do not present as clients in drug treatment clinics but may be in contact with other services, including sexual health services.
Where clinically appropriate, the provision of affordable and accessible pre-exposure prophylaxis for HIV prevention for all in need of it, including people who use drugs, is supported by the EUDA and ECDC guidelines as one element of a combination of prevention services. Nonetheless, the evidence on the optimised use of pre-exposure prophylaxis for people who inject drugs is still building. Following potential exposure events, the guidelines also support access to post-exposure prophylaxis for HIV. Lower-threshold services aiming to provide pre- and post-exposure prophylaxis can often face difficulty funding the treatments, which can present a challenge to prevention efforts where these treatments are clinically indicated.
Providing effective harm reduction responses for people exposed to these drug-related risk factors remains a challenge, and the development of tailored interventions is needed. In Europe, treatment services for drug and sexual health problems are usually funded separately, have different eligibility criteria and are rarely co-located. This makes it difficult to provide integrated care for people exposed to the dual risks of unprotected sex and high-risk drug use in the context of sexualised drug use.
Greater investment needed for European drug services to meet WHO targets
EU policymakers have made a commitment to the WHO global health sector strategies to end AIDS and the epidemics of viral hepatitis and sexually transmitted infections by 2030. Achieving these objectives, however, still requires increased investment in harm reduction services, testing and linkage to treatment, as the provision in many countries remains insufficient. Greater efforts are therefore needed to prevent future outbreaks and reduce transmission, thereby reducing the burden of disease associated with HIV, HCV, HBV and other infections among people who inject drugs.
The joint EUDA-ECDC guidance on the prevention and control of infectious diseases among people who inject drugs supports the implementation of tailored community-based prevention, testing and treatment services. This includes testing outside of formal healthcare settings, for example, in outreach services, and highlights how a more integrated approach to testing and linkage to care is an effective way to reduce persistent health inequity. Inclusive harm reduction approaches, particularly the provision of sterile injecting equipment, including in prisons and through pharmacies, are now seen as fundamental to reducing the transmission of infectious diseases among people who inject drugs. However, coverage and access to free needle and syringe provision remain insufficient in many countries, with only 7 of the 25 countries with available data achieving the WHO service provision targets in 2023 (Figure 10.2). There remains a need for policymakers to make the provision of secure funding for harm reduction services working with people who inject drugs a key public health priority.
Figure 10.3. Availability of needle syringe programmes in Europe at regional level, 2023 or the most recent year available
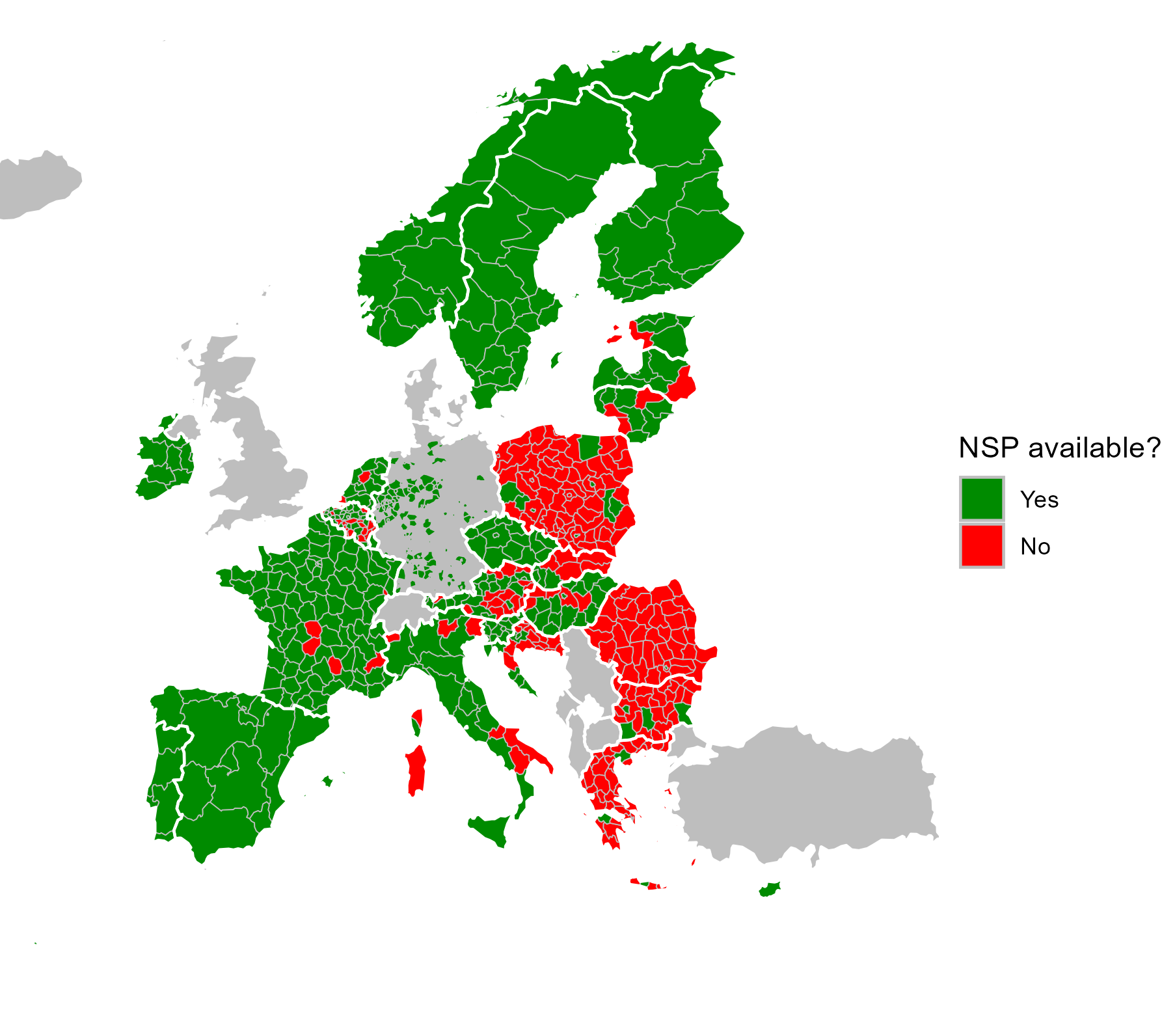
Data are at NUTS levels 2 or 3. For information on NUTS (nomenclature of territorial units for statistics), visit the Eurostat website. The lack of data at NUTS levels 2 or 3 does not mean that the intervention is not available within a country.
Key data and trends
HIV/AIDS
- In 2023, the number of new HIV notifications linked to injecting drug use in the European Union decreased to 980 (2.18 per million inhabitants), compared with 1088 the previous year (Figure 10‑5).
- Ireland, Greece, Cyprus, Latvia, Lithuania and Luxembourg reported a HIV notification rate attributable to injecting drug use higher than 5 per million inhabitants.
- New HIV cases related to injecting drug use accounted for 5.6 % of all new notifications with a known route of transmission in 2023. In the same year, HIV cases related to injecting drug use accounted for more than 10 % of new notifications in Latvia (24 %), Lithuania (19 %), Greece (19 %), Austria (14 %), Finland (12 %), Germany (11 %) and Norway (11 %).
- In 2023, 186 new AIDS diagnoses related to injecting drug use were notified in the European Union, with notification rates highest in Bulgaria, Greece, Cyprus, Latvia, Lithuania and Romania.
HCV and HBV
- Six European countries have recent subnational prevalence estimates of active HCV infection among people who inject drugs and access harm reduction services. The prevalence of active HCV infection derived from seroprevalence studies ranged from just under 7 % in Oslo (2023) to 56 % in Tallinn (2022). Intermediate levels were observed in Madrid (2022) at 20 %, Budapest (2021) at 24 %, Bavaria (2022) at 27 %, and Stockholm (2021) at 30 %.
- In 2023, people who inject drugs continued to face clinical or financial restrictions in accessing direct-acting antiviral HCV treatment in 4 EU Member States.
- Estimates for HBV infection (as measured by the presence of the hepatitis B surface antigen), derived from the latest seroprevalence studies among people who inject drugs, were highest in Hungary (5.8 % in 2021), Latvia (5.6 % in 2022) and Romania (5.6 % in 2023).
- In 2023, there were 20 EU Member States with a viral hepatitis policy that included people who inject drugs. Integrating testing and treatment for HCV, HBV and HIV into harm reduction, drug treatment and prison health services is key to achieving the continuum of care targets for people who inject drugs.
Additional detailed information can be found in the EUDA’s Drug-related infectious diseases: health and social responses.
Source data
The complete set of source data for the European Drug Report 2025, including metadata and methodological notes, is available in our data catalogue.
A subset of this data, used to generate infographics, charts and similar elements on this page, may be found below.
