








Action framework for developing and implementing health and social responses to drug problems
Introduction
The action framework introduced here will help to clarify current thinking about the response process and the factors to take into account at each stage. This will be of particular interest to those planning health and social policy or interventions to address drug problems, but can equally apply to responses at the individual level.
It also provides a structure to the different miniguides which, together, make up the Health and social responses to drug problems: a European guide.
Last update: 18 October 2021.
Contents:






Overview
- Health and social responses to drug problems in Europe are carried out within the context of EU, national and local policies and legal frameworks, and these factors influence the selection and implementation of interventions.
- Responses must adhere to a set of key principles, for example, respect for human rights, including the right to the highest attainable standard of physical and mental health.
- Developing and implementing responses to drug problems, whether at EU, national, local or individual level, involves three basic steps:
- identifying the nature of the problems to be addressed;
- selecting potentially effective interventions to tackle these problems; and
- implementing, monitoring and evaluating the impact of these interventions.
- Many different factors need to be considered at each stage; some of the most important are highlighted here.
The harms associated with drug use depend on the type of drugs involved and how they are used, by whom and in what settings. The many different ways in which these factors can interact result in a wide array of possible drug use scenarios, which are associated with health and social effects of varying severity. The most common combinations of forms of drug use, the profiles of people who use drugs and the settings in which drug use occurs vary between countries across Europe, and, as a result, so do the nature and extent of their drug problems.
As well as differing between countries, drug use and its associated problems may change over time. This means that there can be no single blueprint for tackling drug problems, and that those tasked with responding to these challenges need to regularly review the provision of services available and adapt existing interventions or develop new ones to meet changing needs. Also indicated is the need for a systematic approach, in which the evaluation of effectiveness is integrated into the development, implementation and monitoring of responses to drug problems.
Here we introduce the main issues to be considered in the development and implementation of health and social responses to drug problems. We also outline the framework around which Health and social responses to drug problems: a European guide is structured. The action framework is designed as an aid for those involved in developing and implementing health and social interventions and to serve as a conceptual checklist when reviewing current policy or practice or developing new activities.
A framework for developing health and social responses to drug problems
Health and Social Responses to Drug Problems: A European guide 2021 provides a reference point for those planning or delivering health and social responses to drug problems in Europe. The most appropriate responses will depend on the nature of specific drug problems, the contexts in which they occur and the types of intervention that are both possible and socially acceptable. By providing key information on some of the most important drug issues in Europe and possible responses, the guide aims to assist those involved in tackling these challenges to develop new programmes and improve existing ones.
The action framework introduced here will help to clarify current thinking about the response process and the factors to consider at each stage. This will be of particular interest to those planning health and social policy or interventions to address drug problems, but can equally apply to responses at the individual level.
The framework also provides a structure to the different components of Health and social responses to drug problems: a European guide, which look at health and social responses to a range of drug problems in Europe from three different perspectives: types and patterns of drug use; the role of different settings; and the needs of particular groups. Inevitably, there are overlaps between these different perspectives and the most important are highlighted.
Three stages to developing responses to drug problems
Drug use, and its associated problems, is a complex and multifaceted phenomenon that changes over time. Therefore, the responses required to prevent and mitigate the associated harms to individuals and societies are, of necessity, many and varied. Moreover, they need to have the flexibility to adapt to changing patterns of drug use and the resulting problems, as well as to different national contexts.
The process of responding to drug problems can be divided into three broad stages (Figure 1): the identification of the particular drug problems to be addressed; the selection of the responses or interventions that are to be put in place; and the implementation of these interventions, with monitoring and impact evaluation forming an integral part of this phase. This approach can be applied when developing responses at any level — national, local or system. Equally, these same basic processes apply whether developing a response to a particular problem for the first time or reviewing current provision. While not the primary focus here, the same broad steps — problem identification or needs assessment; response or intervention selection; and implementation and review — are also pertinent when working with individual who use drugs.
In all cases, the starting point should be obtaining an understanding of the extent and nature of the problems to be tackled, which may then be translated into objectives for change. This understanding may be derived from reviewing the available data on the problem, ranging from national statistics to local research and needs assessments, and consulting with stakeholders, including people who use drugs and their closest contacts. The selection of priorities and intervention objectives will stem from the problem definition and be informed by public and political attitudes, as well as local and national priorities.

In the second stage, decisions are made with regard to the actions that should be taken and plans are formulated to implement them. Factors to be considered at this point are the types of intervention that are likely to be effective, the target groups involved, and the settings in which the measures will be carried out. Depending on the circumstances, this might involve selecting from a range of intervention options where there is evidence of effectiveness; adopting and adapting interventions that have been shown to work elsewhere; or extending or optimising existing evidence-based interventions. If no suitable options exist, this phase of the process may involve developing a new intervention. Where a programme or strategy is already in place, it may be necessary to review provision in light of the needs of particular groups or to fill gaps in coverage. These decisions will be influenced by considerations such as the scale and severity of the problem, the resources and competencies available, the outcomes expected, and the values and preferences of the community.
Once suitable responses have been chosen, the next stage is implementation. Whether an evidence-based intervention works in a particular case will depend on how it is put into practice as well as the local context. Therefore, an essential component in this phase is the monitoring and evaluation of the implementation, including the costs and outcomes, to feed back into an ongoing review and planning process.
Overarching context and key principles
Various international policies and papers — including the Common Position on UNGASS, the EU drug strategy and other EU documents, such as the minimum quality standards for demand reduction — highlight a number of key principles for health and social responses to drug problems. For the purpose of the guide, we have identified those which are central to responses in this area (see box: Key principles for health and social responses to drug problems in Europe). These principles are fundamental to all health and social responses and will be discussed in different contexts in several components of Health and social responses to drug problems: a European guide.
Both a country’s legal framework and the law enforcement activities it pursues can have a major impact on health and social responses, acting as either a barrier to or a facilitator of these interventions (see box: Key policies and legal frameworks). For example, enforcement activity that focuses on people who use drugs may inhibit help-seeking, while drug control activities may exacerbate the harms associated with use and pose a barrier to the efficient and effective operation of health and social services. On the other hand, employment legislation preventing discrimination against people with a history of drug problems may promote social reintegration and improve the effectiveness of treatment and rehabilitation programmes. The legislative and policy approaches of EU Member States, which vary considerably, can thus have a big impact on the health and social responses adopted and resourced, as well as on their effectiveness.
Problem definition and needs assessment
Defining the problem or making a needs assessment may be undertaken at different levels and by a variety of actors, including public authorities, planners, consultants or practitioners. Various approaches are possible and numerous tools are available to assist in the process, for example, the
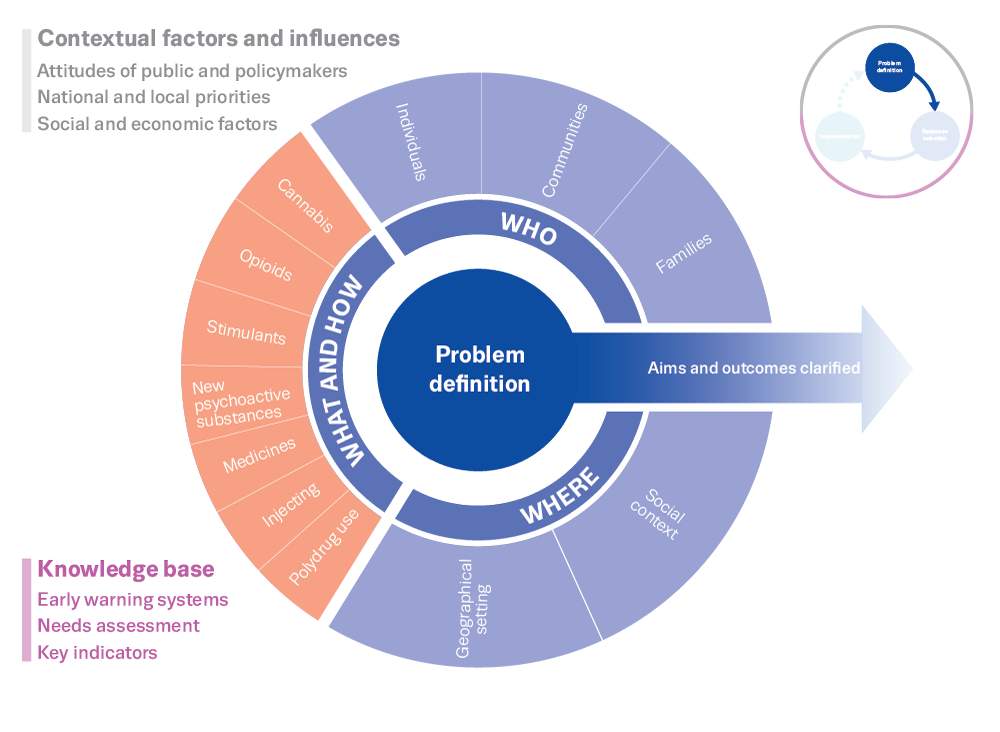
A number of key questions need to be addressed at the initial assessment stage: who is affected; what types of substances and patterns of use are involved; and where is the problem occurring? Responses must be tailored to the particular drug problems being experienced, and these may differ between countries and over time. The wide array of factors that have to be considered at this stage in the process are discussed in this section and illustrated in Figure 2.
Understanding problems arising from particular types or patterns of drug use
Psychoactive drugs act on the brain, producing a variety of changes in perception, mood, thinking and behaviour. Initially these effects may be positive, for example relieving pain or mental distress, or producing pleasure, but they may also lead to a range of harms — either as a result of the direct toxic effects of the substance on the body or through intoxication, as drugs may induce a state of euphoria while impairing rational thinking and physical coordination. If an intoxicated person drives a car, operates machinery or engages in physical activities, they may injure themselves or others, and even, on occasion, cause death. Intoxicated people may also engage in violent acts, either in domestic settings or in social situations that facilitate such behaviour, such as bars crowded with other intoxicated individuals. Chronic drug use, especially sustained daily use, can produce a dependence syndrome, in which people can find it difficult to cut down or stop using a particular drug, despite the damage being done to their health and well-being and that of their family and friends. If such drug use is sustained, it can produce or exacerbate the symptoms of mental and physical disorders and lead to failures in the performance of important social functions, such as attending school, working or caring for children. Among those whose drug use has progressed to dependence, mental health issues and physical comorbidities are common, and many will experience problems in maintaining regular employment or secure housing.
Drug problems may vary according to the type of drug involved, the route of administration (e.g. taken orally, smoked or injected) and the frequency or pattern of use. These variables interact with other factors, such as the characteristics of the person using the drug (e.g. young people, women or men, socially integrated or disadvantaged people) and the social settings in which the drugs are taken (e.g. the workplace, at home, in a nightclub or bar, on the streets), to either increase or reduce the problems that people who use drugs experience. It is thus important to identify which of these factors are relevant when developing interventions to address drug problems.
Pinpointing the main problem drugs and patterns of use will indicate the probable major associated harms. Heroin and pharmaceutical opioids have a high dependence risk, especially if injected. Their use can lead to fatal overdoses, and if people share contaminated injection equipment they risk contracting and spreading blood-borne infections such as HIV and hepatitis B and C.
Stimulants, such as cocaine, MDMA and amphetamines, intoxicate. These drugs are often used recreationally, but may be associated with more problematic patterns of use and modes of ingestion, such as injection or smoking. People under the influence of these substances may engage in risky sexual behaviours and other activities (e.g. driving a car) that puts their safety and that of others at risk. When stimulants are used over weeks or months in high doses, they may precipitate psychoses and serious cardiovascular events, such as heart attacks and strokes. In the case of some stimulants, such as MDMA, fatal or very serious harms may result from a single high-strength dose, and as such are not necessarily associated with regular use.
Cannabis has a very low risk of fatal outcomes, but its use can be associated with acute toxicity presentations at hospital. The risk of developing dependence on cannabis is estimated to be lower than is the case with opioids, or legal drugs like alcohol and tobacco. Nonetheless, people who use cannabis regularly may develop problem use and seek help to stop using. In addition, regular or early use of cannabis is thought to be associated with increased risks of developing mental health disorders or experiencing social and educational problems.
People who use drugs regularly tend to take more than one substance. Most engage in polydrug use — the use of multiple drugs, in combination or at different times. For example, people who inject heroin often use other opioids, alcohol, tobacco, benzodiazepines, cannabis and stimulants. People who use cocaine tend to take it alongside alcohol. Many people who use cannabis daily also smoke tobacco. These drug combinations can exacerbate the risk of harm, for example by increasing the likelihood of toxic drug effects, fatal overdoses or developing dependence on multiple drugs, which can be more difficult to overcome than dependence on a single drug.
Understanding the role of different settings
The setting in which drugs are used must be considered, as this can affect the type and extent of harm that drug use can cause. Those who take drugs when they are alone may be at higher risk of some harms; in particular, there will be no one to help them if they experience a drug overdose. Using opioids while alone, for example, increases the risk of a fatal overdose.
People who use drugs in public places often do so furtively and hurriedly. This can increase the risk of an overdose or of acquiring a blood-borne viral infection if they are sharing injecting equipment. Poor hygiene, often associated with such settings, also increases the risk of a range of infections. This is a particular issue for homeless people. Drug use in prisons is also clandestine and risky (see also Opioids: health and social responses, Drug-related infectious diseases: health and social responses).
In relation to recreational settings, using MDMA in a hot nightclub, for example, may put a person who is already predisposed to hyperthermia at greater risk of experiencing this rare but serious adverse outcome. More generally, the use of drugs in the workplace can pose safety risks, for example when using machinery or driving under the influence.
Understanding the harms to individuals and communities
An important step in defining the problem is identifying the most important drivers (or causal factors) for harms, and which individuals or communities are principally affected. For example, is there a problem due to increasing cannabis use among young people? And if so, is this concentrated within a particular age group, community or geographical area? Further, is this increase in cannabis use associated with school drop-out rates, rising youth unemployment, or increasing mental health problems? Answering these types of questions will clarify the issues to address, the outcomes to be sought and the criteria against which to measure the impact of the intervention.
An array of individual and societal factors can make some people who use drugs more vulnerable to harm. This is also true with respect to the families and communities affected by drug problems. These factors interact in complex ways to reduce or increase the risks and harms associated with drug use. In addition, they may act together with drug use in a circular fashion to create a vicious cycle. Some of the key components that need to be considered, along with their impact on the harms associated with drug use, are summarised in the box ‘Examples of factors to consider when assessing drug problems’. More information is provided throughout the different components of the guide.
Identifying and prioritising the problems to be tackled
Needs assessment is likely to identify a range of potential problems to be addressed. In deciding which problems to tackle, a public health approach is useful. This approach first assesses the severity of the problems experienced by people who use drugs. The next step in the process is looking for interventions that will reduce the impact of the drug problems that have been identified. This approach identifies priority areas for action based on the evidence, but is also influenced to some extent by political and public attitudes.
For example, in many European countries, drug overdose deaths are a major cause of mortality among men aged between 25 and 55, and in some areas are increasing, with heroin or other opioids implicated in the majority of these deaths. These premature deaths have a huge impact on families (who lose parents, children or siblings), as well as the wider society, and place major demands on emergency health services. Reducing opioid-related deaths is therefore a high public health priority in terms of the drug policies in many jurisdictions.
Deaths and other adverse events associated with new psychoactive substances often generate considerable media attention and public concern. Although such events are rare, tackling the harms associated with the use of these substances, which pose unknown risks to people who use drugs, is a priority across Europe.
Another issue of concern is the presence of open drug scenes, where drug use and dealing take place in public spaces. These scenes, associated with public nuisance and the potential for violence, often generate public concern, and may be a priority for intervention. Responses here need to consider the needs of both the local communities and the people engaged in high-risk drug use.
Developing appropriate health and social responses
Clarifying the objectives for the interventions
Having defined the drug problems that need to be tackled, the next step is to identify the responses that are likely to be effective in dealing with them. Where appropriate, a combination of interventions may be used, as individual measures are rarely sufficient. Choosing the appropriate responses requires a clear understanding of the primary objectives of the interventions. For example, the goals might be one or more of the following:
- to prevent young people from initiating drug use;
- to delay the age when people initiate drug use;
- to prevent experimental drug use from becoming regular use;
- to help people stop using drugs;
- to reduce drug use and harm among people who are already using drugs;
- to reduce the drug-related harms experienced by communities; or
- to increase the social integration of people with drug problems.
The aims will depend upon a combination of factors, including an assessment of the nature and stage of development of the drug problem to be addressed, for example:
- Is a new drug beginning to cause problems although the number of people who use it is still relatively small?
- Is an established drug like heroin, with many people engaged in high-risk drug use, causing new problems or are the interventions in place failing to adequately address long-standing harms?
- Are there concerns about the resurgence of an illicit drug such as MDMA?
In the case of a new psychoactive substance, the aim may be to discourage young people from experimentation, or to encourage those who have started using to stop or not to use regularly, while avoiding giving the impression that the use of such drugs is the norm. Research may be needed to identify problematic patterns of use with regard to new drugs. Health educators may need to explore effective and targeted ways of informing people who use drugs about the potential harms and riskiest patterns of drug use, such as peer-based interventions or messaging in selected and trusted social media channels.
In the case of an established drug, the objective may be to prevent new drug use while encouraging people already using and experiencing problems to engage with drug services.
Understanding and using evidence
Different types of evidence may be used in developing and implementing responses. This can include:
- evaluations of interventions, such as randomised controlled trials and other experimental designs or observational studies. These can help assess the quality of the evidence and the direction of each intervention’s effect (beneficial or not);
- implementation studies, which investigate which factors have been found to be associated with effective service provision;
- syntheses of expert opinion from stakeholders. This can be used, for example, in guideline development (to complement other forms of evidence). Ideally this should include input from both those involved in the intervention’s delivery and its potential recipients.
- Basic science and research findings that can inform the design of new interventions.
The various types of evidence differ in their strengths and weaknesses and in the information they can provide. Drug-related problems are multifaceted and require not only medical but also socioeconomic and educational interventions. As a result, it is often necessary to integrate evidence from a range of disciplines and types of study, using both quantitative and qualitative research methods.
In reviewing what evidence is available to inform decision-making, the first step is to define the research question, which in turn determines the most appropriate study design. For example, the effectiveness of treatment on individuals is usually best evaluated through randomised controlled trials. To determine the longer-term impact of an intervention that has already proved to be effective or the impact of broader policies or population-based interventions, observational studies are likely to be more appropriate. These include, for example, longitudinal or cohort studies, interrupted time series or controlled before-and-after studies.
It is also important to consider the quality and relevance of the available evidence. Are the findings taken from appropriately designed studies and based on well-conducted research that minimises biases? Are they reported correctly and related to the target groups of interest?
There are a number of ways of evaluating the quality of the available evidence. The best evidence comes from systematic reviews that combine the results of multiple studies and assess their quality as well as the extent to which they show consistent findings. However, in emerging fields it can take some time for sufficient primary studies to be completed and systematic reviews undertaken, meaning that services will often need to be developed in areas where the evidence base is weak or partial.
When using evidence, it is also important to recognise that the quality of the evidence is not the only consideration, as there can be interventions that have shown effective results but for which the evidence is currently weak because they have not yet been sufficiently researched. Similarly, there can be high-quality evidence of an intervention being effective, but with only a small beneficial effect. Importantly, evidence statements are not broadly applicable but linked to specific outcomes and, usually, specific populations, settings, or both. Therefore, understanding how outcomes have been defined and measured is crucial when considering how the evidence available can be interpreted.
Evaluating the evidence used for this guide
The evidence statements in this guide are a compilation of what is known about responding to drug use. They reflect only domains where we have clear evidence to support an intervention. In many situations, the evidence to support an intervention is limited due to a lack of robust evaluation, or because the available evidence has not been synthesised in a way that facilitates an evaluation (i.e., no systematic reviews or meta-analyses of the evidence have been conducted). Lack of evidence, or low-quality evidence, does not necessarily mean that an intervention does not work. It means that the intervention has not yet been adequately evaluated so at this point in time there is a high degree of uncertainty in predicting what impact it will have.
Methodology
In this guide, the evidence statements are based on evidence from systematic reviews and meta-analyses published from January 2010 to March 2021. Systematic reviews and meta-analyses were identified from PubMed searches for each topic using relevant medical subject headings. From the relevant studies identified full-text papers were obtained for the relevant reviews, from which key data were extracted: publication details, the population studied, the intervention evaluated, a description of included studies (that is, the number of trials/participants, types of study design), and quality (study design). Where available, evidence statements and their GRADE quality ratings were extracted and used (Cochrane GRADE). Evidence derived from single studies was rated as ‘very low quality or insufficient evidence’. Where there was more than one review available on a particular topic, evidence statements were based on the most recent robust evidence available and considered the consistency of evidence across reviews. Where evidence was not consistent, a judgement was made regarding the strongest evidence, based on the recency of the review, and on the number and quality of included studies. In some cases, GRADE quality ratings for reviews needed to be re-assessed to maintain consistency across reviews. Evidence from narrative reviews was generally excluded.
Because of the methods used, evidence statements are necessarily constrained to domains where adequate evidence is available to confirm (or refute) the benefits of an intervention. In some cases, good evidence may have been available to demonstrate the benefits of an intervention, but it had not been synthesised in a fashion that allowed the quality of the evidence to be judged (i.e., no systematic reviews or meta-analyses existed). In these situations, evidence regarding that intervention was not included in the evidence statements. In other situations, evidence was available from only a single study, or it was low quality (e.g., due to study design limitations). This meant that the evidence was not conclusive; the quality rating assigned to the evidence statement in these situations was very low or insufficient. In many intervention areas, we do not report on evidence where it was inconclusive or very low quality because of space limitations.
Summarising the evidence
The evidence-based rating system used in this guide has two dimensions. All evidence refers to a specific outcome measured in a specific population and/or setting and timeframe.
The first dimension reflects the direction of the intervention’s effect — that is, whether the intervention has been consistently found to produce a benefit, unclear benefit, or potential harm:
- Beneficial: Evidence of benefit in the intended direction.
- Unclear: Unclear whether the intervention produces the intended benefit.
- Potential harm: Evidence of potential harm, or evidence that the intervention has the opposite effect to that intended (e.g. increasing rather than decreasing drug use).
The second dimension represents the quality of the evidence and is based on the Cochrane GRADE rating system, where the ratings reflect confidence in the quality of the evidence. This is shown through:
- High: We can have a high level of confidence in the evidence available
- Moderate: We are reasonably confident in the evidence available
- Low: We have limited confidence in the evidence available
- Very low: The evidence available is currently insufficient and therefore considerable uncertainty exists as to whether it will produce the intended outcome.
Low or very low-quality evidence will be common for new responses or interventions addressing emerging problems. It is therefore important to include an evaluation and be vigilant for possible adverse or unintended outcomes.
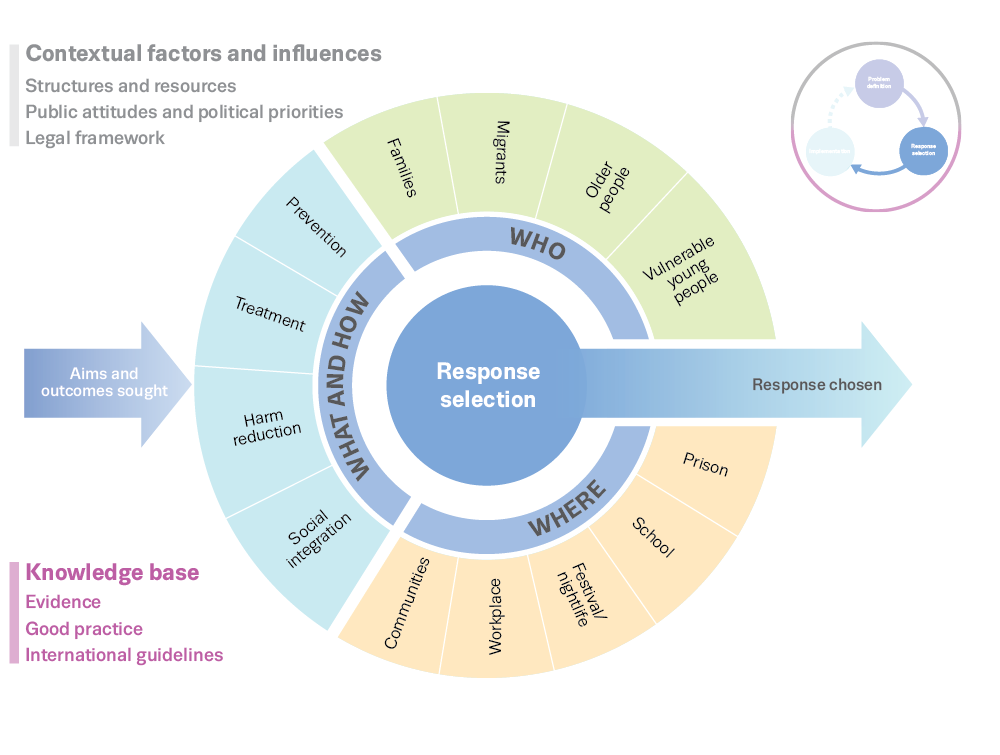
Selecting the most appropriate response options
The next stage, based on the needs assessment and defined objectives, is to decide on an appropriate response. There are potentially three ways to proceed in this regard: extending or improving an existing response; importing an approach or programme that has been used elsewhere; or developing a new intervention. In some cases, the most appropriate tactic may be to slightly modify an existing response (e.g. extending the opening hours of a service or adding a component to a training programme). In other circumstances, a new intervention may be required and a number of factors will have to be considered in selecting the most appropriate and effective response (Figure 3).
The first questions that need to be asked are what response options are available to address the problem and what evidence exists for their effectiveness? Ideally, interventions should be supported by the strongest available evidence, if possible meta-analyses and systematic reviews of large-scale randomised controlled trials and observational studies of treatment outcomes that combine the results of multiple studies involving large numbers of individuals. However, such evidence is not always obtainable, and, at the other end of the spectrum, in cases where data is very limited or non-existent, expert consensus may be the best option until more conclusive evidence can be gathered.
If no suitable responses are available then research may be required to develop an intervention, investigate its feasibility and evaluate its acceptability to the target group. Later, when the programme has been implemented and experience gained in using it, research will be needed to evaluate it.
The main types of available responses and modes of delivery are described briefly in the next section. A combination of response measures will often be required to tackle the multiple aspects of complex problems.
Another factor to be considered at this stage is the specific target group intended to benefit from the intervention. For example, will the programme be delivered to:
- the whole population of people who may potentially use drugs, for example, the adult population;
- subsets of the population who are at higher risk of initiating drug use or who may have particular needs, such as socially disadvantaged youth, homeless people, women, ethnic minority groups; or
- people who are already using drugs or have individual vulnerability?
A final consideration is the setting in which the programme will be delivered, for example, schools, nightlife settings, workplaces, prisons or treatment facilities. These varied settings can both provide opportunities and impose constraints, which must be considered.
In addition to those listed above, other factors need to be considered when making choices about the mix of interventions to implement. These include the available structures and resources for delivering the relevant services. For example:
- Are there government, not-for-profit, civil society and charitable organisations that are already providing these types of services?
- Are the services available at a sufficient scale or, if not, do they have the capacity to expand?
- What additional resources may be required to enable existing services to expand their capacity, for example: funds for new buildings, additional staff and staff training?
At times of limited resources or if there is a need for a rapid response to a crisis, there may have to be a trade-off between the coverage of services (reaching the greatest number of people) and the intensity or level of provision (service quality) that can be offered.
The level of political priority given to the drug problem is an important factor in resource allocation. Is it sufficient to generate the resources needed to expand capacity, or will established service providers be expected to address the new problem with their existing resources? How will decisions be made with regard to prioritising the delivery of services to different clients and allocating resources between various services?
Moreover, public attitudes towards drug use may be a major determinant of political priority, influencing the amount of societal resources allocated to, and the approach taken in addressing drug problems. These attitudes will depend on the prevailing ‘governing images’ of drug use — whether drug use is primarily seen as a vice, a crime, a personal choice, an illness or a disability.
In addition, a country’s drug laws may have an impact on the type of responses provided. In all EU countries, possession of controlled drugs is defined by law as an offence, and in many, use of these drugs is a crime. In principle, those who use illicit drugs can be sentenced to a term in prison, but many countries take a public health approach to the health and social problems arising from drug use, diverting people who use drugs out of the criminal justice system and into treatment. In some countries, this has led to increased funding for treatment and initiatives to address the health and social problems experienced by people who use drugs.
Main types of responses available
A wide range of health and social responses are available for tackling drug problems. These may be used with different populations, at various stages in the drug problem, individually or in combination. When considered at the national or local level, all these measures may form part of a comprehensive drug demand reduction system and will need to be coordinated and integrated. An increasing number of prevention, treatment and harm reduction interventions are now being provided online.
Prevention approaches
Approaches to drug prevention cover a wide spectrum, ranging from those that target society as a whole (environmental prevention) to interventions focusing on at-risk individuals (indicated prevention). The main challenges lie in matching these different strategies to the appropriate target groups and contexts, while ensuring that they are evidence-based and have sufficient population coverage. Most prevention strategies focus on substance use in general, although some also consider associated problems, for instance, violence and high-risk sexual behaviour, with a limited number targeting specific substances, such as alcohol, tobacco or cannabis.
- Environmental prevention strategies aim to change the cultural, social, physical and economic environments in which people make choices about drug use. They include measures such as alcohol pricing and bans on tobacco advertising and smoking, for which there is good evidence of effectiveness. Other strategies aim to provide protective school environments, for example by promoting a positive and supportive learning climate and teaching citizenship norms and values.
- Universal prevention addresses entire populations, usually in school and community settings, with the aim of giving young people the social and personal competences to avoid or delay initiation of substance use.
- Selective prevention intervenes in specific settings or with particular groups, families or communities that are more likely to develop drug use or dependence, often because they have fewer social ties and resources.
- Indicated prevention targets individuals with behavioural or psychological problems that predict a higher risk of substance use problems later in life. In most European countries, indicated prevention primarily involves counselling young people who use drugs.
Treatment
A range of interventions are used for the treatment of drug problems in Europe, including psychosocial interventions, pharmacological treatment and detoxification. The relative importance of the different treatment modalities available is influenced by a number of factors, including the organisation of the national healthcare system and the nature of the drug problems in each country. Drug treatment services may be provided in a variety of outpatient and inpatient settings: specialist treatment units; primary healthcare and mental health clinics; low-threshold agencies; hospital-based residential units and specialist residential centres; or units within prisons.
Most drug treatment in Europe is provided in outpatient settings, and the two main modalities for such services are opioid agonist treatment [1] and psychosocial interventions.
Increasingly, a wide range of treatment interventions are provided online. Internet-based interventions have the potential to extend the reach and geographical coverage of treatment programmes to people experiencing drug use problems who may not otherwise have access to specialist drug services.
Opioid agonist treatment is the predominant intervention for opioid use in Europe. It is generally provided in specialist outpatient settings, although in some countries it is also available in inpatient settings and prisons. In addition, office-based general practitioners play an important role, often through shared-care arrangements with specialist addiction treatment centres.
Psychosocial interventions include counselling, motivational interviewing, cognitive behavioural therapy, case management, group and family therapy, and relapse prevention. These interventions support people in managing and overcoming their drug problems. They are the main form of treatment provided to people who use cannabis and stimulant drugs, such as cocaine and amphetamines. They are also offered to people who use opioids in combination with opioid agonist treatment. In many countries, the responsibility for outpatient psychosocial treatment is shared between public institutions and non-governmental organisations. Commercial providers generally play a minor role in the provision of psychosocial interventions in Europe.
A smaller proportion of drug treatment in Europe is provided in inpatient settings. Inpatient or residential treatment, whether hospital-based or non-hospital-based, requires clients to live in the treatment facility for a period ranging from a few weeks to several months, with a view to enabling them to abstain from drug use. The provision of opioid agonist treatment in inpatient settings is rare, but is undertaken for selected client groups with high levels of morbidity. A prerequisite for entry may be detoxification, a short-term, medically supervised intervention aimed at the reduction and cessation of substance use, with support provided to alleviate withdrawal symptoms or other negative effects. Detoxification is usually provided as an inpatient intervention in hospitals, specialised treatment centres or residential facilities with medical or psychiatric wards.
In inpatient settings, clients receive individually structured psychosocial treatments and take part in activities to rehabilitate them and facilitate their reintegration into society. A therapeutic community approach is often used (see also Opioids: health and social responses). Inpatient treatment may also be provided in psychiatric hospitals for those with comorbid mental health problems. Public institutions, the private sector and non-governmental organisations are all involved in the provision of inpatient care in Europe, with the main providers varying between countries.
[1] The term opioid agonist treatment is used here as preferred language to cover a range of treatments that involve the prescription of opioid agonists to treat opioid dependence. The reader should be aware this term includes opioid substitution treatment (OST), which may still be used in some of our data collection tools and historical documents.
Social reintegration
Social exclusion is experienced by many people engaged in high-risk drug use, especially chronic opioid use. Unemployment and low educational attainment are common among people in this category, and many are homeless or living in unstable accommodation. Interventions addressing these issues focus on the social reintegration of people who use drugs, including improving a person’s ability to gain and maintain employment.
Approaches taken include vocational training programmes that aim to improve the skills and qualities needed to find and secure a job. The transition from treatment into mainstream work may be facilitated by social enterprises and cooperatives that offer work experience and supported employment. Programmes that engage with businesses to encourage them to employ people who have had drug problems and provide in-work support are also valuable.
Addressing housing problems is also often seen as essential in enabling social reintegration. Housing support services may provide short- or long-term accommodation, as well as access to other services such as medical care, drug treatment, social activities, education and training. These services include programmes such as ‘Housing First’, which provides accommodation as quickly as possible before tackling an individual’s drug problem or offering other support.
Harm reduction
Harm reduction encompasses interventions, programmes and policies that seek to reduce the health, social and economic harms caused to individuals, communities and societies by drug use. A core principle of harm reduction is the development of pragmatic responses to dealing with drug use through a hierarchy of intervention goals that place the primary emphasis on reducing the health-related harms of continued drug use. Harm reduction addresses the immediate health and social needs of people experiencing problematic drug use, especially the socially excluded, by offering opioid agonist treatment and needle and syringe programmes to prevent overdose deaths and reduce the likelihood of contracting infectious diseases. Additional approaches include outreach work, health promotion and education.
Protecting both people who use drugs and the public from the harms associated with drug use requires a framework of interventions across different areas of potential harm and risk that can help to achieve better health and social outcomes over time. Important potential targets for interventions in this area include measures to reduce the risk of HIV/AIDS or viral hepatitis infections among people who inject drugs, overdose prevention, and approaches that encourage people who use drugs to adopt less risky behaviours as well as promoting health and safety objectives.
More recent developments in the field of harm reduction interventions include the use of e-health and mobile applications to deliver brief interventions and support treatment more widely, the use of telemedicine, and employing behavioural insights to develop more effective programmes for people who use drugs.
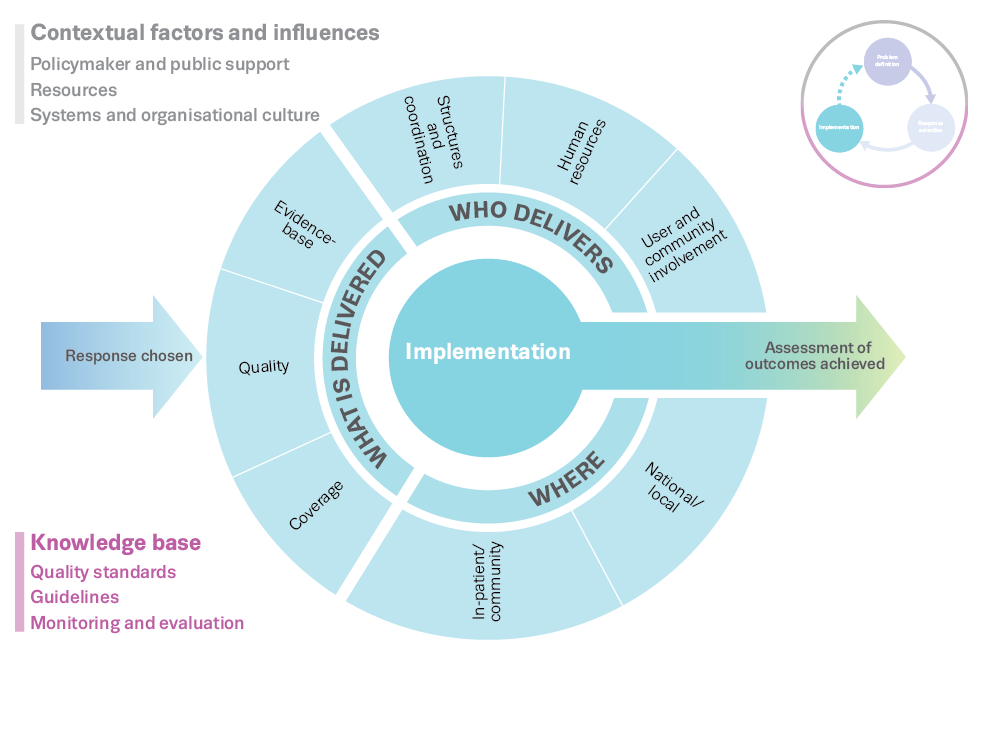
Implementing, monitoring and evaluating the selected responses
Successful implementation of any policy response depends on a range of factors that need to be considered when planning or reviewing policies or programmes (see Figure 4).
Factors affecting implementation
Firstly, enlisting policymaker and public support is essential. Policymakers and the public need to agree that there is a drug problem which requires a specific response. They may also have to be persuaded that a public health approach is more appropriate than a largely public order response. Advocacy that draws attention to the cost-benefits of action and inaction may be needed to ensure the allocation of the societal resources necessary for an effective public policy response.
Effective implementation of an intervention further depends on having sufficient numbers of skilled staff to deliver it. This may require training additional staff to allow services to expand. It may also involve retraining staff more accustomed to dealing with other types of problem drug use (e.g. injecting opioid use rather than problem stimulant or cannabis use) or providing them with the skills to work with new groups, such as younger clients.
Interventions also require appropriate facilities and locations where treatment, outreach activities or other programmes can be conducted. Engaging local communities may be essential if they are to host treatment or outreach services. Concerns that will need to be addressed include fears that the services will attract more people who use drugs to the area and increase drug-related problems, or lead people who use drugs to congregate around treatment centres, openly engaging in drug dealing and drug use.
Management and coordination of services
Management systems are needed to coordinate the efforts of the different agencies and services working to address drug problems. Coordination may require the establishment of advisory committees or reference groups with broad representation from key stakeholders. These bodies can determine the direction of an overall strategy. They can also ensure the involvement of all those affected by a policy, which facilitates wider acceptance of the approaches involved.
In addition, the interaction between drug issues and other health and social problems means that it is important to ensure proper coordination is achieved between drug services and other healthcare provision. For example, drug problems are often associated with mental health issues, and it is therefore essential that drug and mental health services work together to ensure that both concerns are addressed effectively (see Spotlight on… Comorbid substance use and mental health problems).
Quality standards for service provision provide another mechanism for assisting effective implementation. The EU has published minimum quality standards in drug demand reduction that cover prevention, risk and harm reduction and treatment, as well as social reintegration and rehabilitation.
Regular consultations with the agencies involved in service delivery may be needed in order to identify and address any implementation problems. Representatives of groups who use a particular service can provide feedback on its performance and make suggestions for improvements in terms of design and delivery. It is critical to create an organisational culture in which there is collaboration between agencies and service providers rather than competition for resources and clients.
Monitoring and evaluation of service delivery
Monitoring, evaluation and feedback are essential for good service delivery. Such procedures enable staff to monitor the performance of their programmes, improve delivery, assess cost-efficiency and account to funders for the services they deliver. They also allow service providers to identify any unintended negative consequences of particular interventions or other actions, for example a change in practice leading to higher drop-out rates, or where steps taken to prevent the diversion of prescription medicines reduce access for patients who require them, leading to ineffective treatment and associated pain and suffering, as well as increased healthcare costs.
Monitoring the implementation and uptake of interventions requires the establishment of sustainable data collection systems. If the data are to be useful, forms need to be routinely and properly completed. Results should be fed back to staff to demonstrate the value of data collection. Examples of the types of questions that need to be asked in monitoring and evaluating interventions are:
- What types of intervention have been delivered (e.g. counselling, social support, opioid agonist treatment)?
- How many and what types of clients or target groups have they served?
- What are the outcomes in terms of preventing or reducing drug use and drug-related harm or improving clients’ quality of life?
- How do the interventions’ costs compare to alternative programmes or services?
These data are valuable for both internal and external purposes, for example: evaluating and refining services and responses to clients; reporting to funding bodies; making the case for continued or additional funding for current services; or arguing for alternative, more cost-effective interventions. The monitoring and assessment of ongoing service delivery is usually undertaken by the service providers themselves, while outcome and impact evaluation is ideally undertaken by external evaluators, who can be more objective.
As there may be a delay before interventions have any detectable effects on drug-related harm, a potential challenge for policymakers is to ensure that services continue to be funded when a perceived drug crisis has passed. Research findings on the impact of services, their cost-effectiveness and the scale of drug problems at the population level can play a useful role in this process.
Further resources
EMCDDA
- Best practice portal.
- Drug-related public expenditure.
- Implementing quality standards for drug services and systems: a six-step guide to support quality assurance, EMCDDA Manual, 2021.
- Drug prevention: exploring a systems approach, 2019.
- European Prevention Curriculum (EUPC): a handbook for decision-makers, opinion-makers and policy-makers in science-based prevention of substance use, EMCDDA Manual, 2019.
- Drug treatment expenditure: a methodological overview, EMCDDA Insights, 2017.
- New developments in national drug strategies in Europe, 2017.
- Evidence review summary: drug demand reduction, treatment, and harm reduction, Harry Sumnall, Geoff Bates and Lisa Jones, background paper, 2017.
Other sources
- EU drug strategy (2021–2025).
- EU action plan on drugs 2021-2025.
- EU Common Position on UNGASS, 2016.
- EU Minimum quality standards for demand reduction, 2015.
About this publication
Recommended citation: European Monitoring Centre for Drugs and Drug Addiction (2021), Action framework for developing and implementing health and social responses to drug problems, https://www.emcdda.europa.eu/publications/mini-guides/action-framework-….
Identifiers
TD-02-21-996-EN-Q
ISBN: 978-92-9497-671-0
DOI: 10.2810/693826